Talk Blue Vlaanderen, Flemish patient association for people with intestinal cancer.
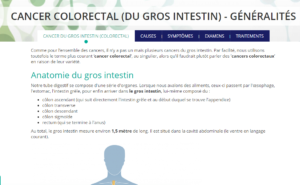
Intestinal cancer is the collective name for several cancer types in the intestinal system. The intestines consist of three parts: the lower intestine, the colon and the rectum. A term that is often used for intestinal cancer is colorectal cancer (CRC): the vast majority of cases concern the colon and the rectum.
Most commonly, a colorectal tumour starts off as a benign polyp in the intestinal wall. A benign polyp is a growth of cells that can vary in shape or size. Often people can have one or more polyps in their intestines without knowing: it is estimated that between 5 and 20% of all adults over 50 years old has polyps. Once the cells in these growths display uncontrolled growth, we call it cancer.
Survivability of colorectal cancer greatly benefits from an early diagnosis. This is why all Belgian men and women between the ages of 53 and 74 years old are invited to be screened for colon cancer biannually. Colon cancer is one of the most frequently occurring cancer types in Belgium, affecting roughly 5% of the population.
Colon cancer
The colon is part of the digestive system: it compresses food that has been processed by the small intestine while extracting nutrients, salt and water. Colon cancer occurs most often as a benign polyp on the right hand side of the body, where the sigmoid colon moves down towards the rectum.
Rectum cancer
The rectum is another name for the last part of the colon, and is about 15 centimetres in length. This part of the colon is closed off by a sphincter muscle on either side, and it serves as a temporary deposit for faeces. Once the rectum reaches capacity level, an impulse signal is triggered so people experience the urge to go to the toilet.
Of all colorectal cancer patients, roughly 30% has rectum cancer.
Cancers of the small intestine
Cancer in the small intestine is relatively rare compared to colorectal cancer. In 2015, 315 new cases of small intestine cancer were diagnosed on a total of 67,087 cancer patients. This type of cancer mostly targets elderly patients.
The small intestine consists of three parts, starting with the duodenum, where food arrives from the stomach and gets mixed with enzymes from the pancreas and the gall bladder. The next and longest part of the small intestine is called the jejunum: here most of the nutrients are absorbed from the food. The ileum forms the final tract of the small intestine, this is where vitamin B12 is absorbed before the food passes on to the colon.
Unlike colorectal cancer, that virtually always grows from polyps, small intestine cancer can occur in several distinct forms.
More information on leiomyosarcoma and gastrointestinal stromal tumours can be found at their specific Oncopedia entries.
Most common symptoms in patients with intestinal cancer are:
As is so often the case with cancer, there is no clear cause for intestinal cancer. But certain risk factors have been identified that carry an enlarged risk of contracting the disease:
When a patient presents symptoms such as constipation and blood in faeces, chances are a GP will immediately suspect colon cancer. In order to make sure, the GP will conduct further tests, like a blood test and a rectal exam. Subsequently, the patient will be referred to a specialist, who will perform further tests. These will almost certainly include a colonoscopy, in which the intestinal walls are examined using a flexible tube and a micro camera, which is inserted anally. If small intestine cancer is suspected, the specialist may opt for a duodenoscopy, where a tube with a micro camera is introduced orally. In both tests, a biopsy can be performed for further examination.
Other test methods are a CT colonography, for instance in cases where the colonoscopy could not reach the affected area of the colon. Additional blood work will help to establish the CEA levels. CEA stands for carcinoembryonic antigens. These antigen levels are raised in patients with colon cancer.
If colon cancer has been established, further tests are conducted in order to determine the cancer stage. This is necessary when it comes to devising a treatment plan and a prognosis. These tests include CT scans, pulmonary X-rays, blood work, MRI, FDG and PET scans.
In determining the stage of intestinal cancer, the TNM classification system is used. The T stands for the state of the primary tumour; N denotes the amount of spreading to the lymph nodes; and M stands for metastasis to other organs. This leads to the following classification hierarchy:
The differentiation of the tumour is an important factor in establishing a prognosis and treatment. This can be determined on the basis of a biopsy. A biopsy involves the removal of a small bit of tissue that can be examined under a microscope. Differentiation determines the degree of mutation in the cancerous cells.
The development stage of the cancer strongly determines the treatment strategy. In case the cancer is diagnosed at an early stage, it can sometimes be an option to remove the cancerous polyps during the colonoscopy procedure. Based on the results of tissue research, further treatments may be offered. Often, the cancer has progressed beyond these early stages, in which case operation is the go-to treatment, during which the affected part of the colon is surgically removed, along with fatty tissue that may contain lymph nodes. Operation can be followed up by chemotherapy.
Should the tumour spread, other treatments or combinations are available. These include:
How and which treatments are combined depends on the type of intestinal cancer. Chemotherapy is commonly prescribed as a post-operative therapy for stage III colon cancer patients, but not for patients with rectum cancer. The reason is that colon cancer carries a high risk of metastasis, even after treatment, whereas rectum cancer does not.